
Cervical Myelopathy: When the Spinal Cord Is Running Out of Room
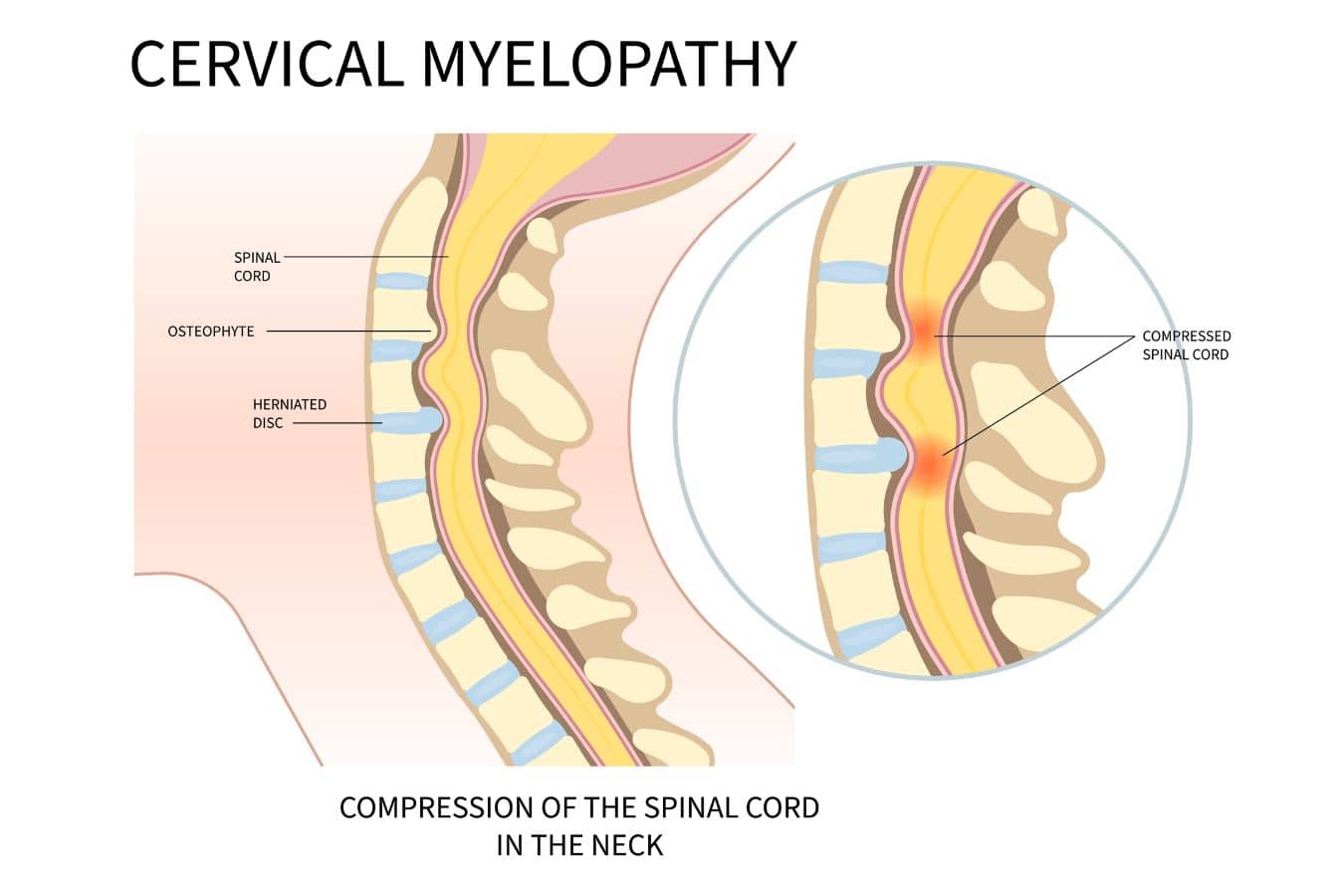
Cervical myelopathy is a condition where the spinal cord in the neck is being compressed, usually by a combination of disc bulging, bone spur formation, and thickening of the ligaments that occurs with age. The compression gradually impairs the spinal cord’s ability to transmit signals to the arms, hands, and legs. It is the most common cause of spinal cord dysfunction in adults over 50.
I want to start by addressing something patients hear a lot: “You could become paralyzed if you don’t have surgery.” That framing is common, but the reality is more nuanced than that.




How myelopathy actually progresses
In the setting of regular daily life, cervical myelopathy progresses slowly. It is not a condition where you are fine one day and paralyzed the next. Most patients notice a gradual change: their hands feel clumsy, their handwriting gets worse, buttons become harder to fasten, their balance feels off, or their legs feel heavy when they walk. Sometimes they have trouble emptying their bladder. These symptoms tend to develop over months or years, not days.
There is one important exception. If you have a narrowed spinal canal from cervical stenosis and you sustain a hyperextension injury, a fall, a car accident, anything that snaps the neck backward, the canal diameter decreases instantaneously and the spinal cord can be acutely injured. This is a real risk, and it’s one of the reasons we take significant stenosis seriously even in patients whose day-to-day symptoms are mild. But this acute scenario is different from the slow, degenerative progression that most myelopathy patients experience.
The fear-based messaging around myelopathy leads to two problems. Some patients feel rushed into surgery they may not need yet. Others avoid seeing a surgeon entirely because they’re afraid of what they’ll be told. Neither is a good outcome. And if a patient does want to have surgery to mitigate the risk of a future fall or accident, that is reasonable, as long as they are making an informed decision in concert with their surgeon.

Call today to Schedule your Consultation
Dr. Alexander Taghva delivers advanced spine and brain solutions.
When I recommend surgery
There is a lot of ongoing discussion in academic spine circles about when to operate on cervical myelopathy, and the field has actually become more conservative over the past decade. Not every patient with imaging findings of cord compression needs surgery. Some patients have mild stenosis, no symptoms, and may never progress.
My own guidelines for recommending surgery are:
When there is cord signal change on MRI. This bright signal inside the spinal cord on T2-weighted images represents edema or gliosis, and it tells me the cord is being damaged at a cellular level. In my experience, this finding tips the balance toward surgery even if the patient’s symptoms are still relatively mild.
When neurologic symptoms become consistent, progressive, or disabling. This includes gait instability that isn’t improving, hand weakness or clumsiness that’s getting worse, difficulty with fine motor tasks, or urinary retention. Isolated mild symptoms that have been stable for a year are a different conversation than symptoms that are clearly worsening over months. A litmus test we often use for patients is – if these symptoms were to become permanent, could you live with that?
The reason I lean toward earlier surgery in patients who meet these criteria is that the outcomes are better when we intervene before the cord has sustained irreversible damage. The spinal cord has limited ability to recover once it’s been compressed for a long time. Patients who undergo surgery while their deficits are still mild tend to improve. Patients who wait until they can barely walk have a lower ceiling for recovery.

The uncomfortable calculation
I want to be transparent about something that surgeons don’t always say out loud. Part of the decision to operate on cervical myelopathy involves thinking about trajectory. How old is the patient? How fast are they declining? How long are they likely to live? What is the immediate surgical risk versus the long-term risk of progressive neurologic decline?
A 55-year-old with early myelopathy and cord signal change has decades of life ahead and a slow compression that will almost certainly get worse. Surgery makes sense. A 90-year-old with mild symptoms, significant medical comorbidities, and a moderate stenosis requires a very different conversation. The surgery itself carries real risk, particularly in older patients, and the disease may never progress enough to matter in their remaining years.
This is not a comfortable calculation. But it’s the honest one. And patients deserve to be part of it rather than just being told “you need surgery” or “you’re fine” without understanding the reasoning.


-

- Julie Lytle



Surgical options
There is no single operation for cervical myelopathy. The choice depends on where the compression is coming from, how many levels are involved, and the alignment of the cervical spine.

Anterior cervical discectomy and fusion (ACDF)
This is the approach when compression is primarily from the front, from disc herniations or bone spurs pushing backward into the spinal cord. We go through a small incision in the front of the neck, remove the disc and any bone spurs, decompress the cord and nerve roots, and fuse the segment with a cage or bone graft. Sometimes removing more of the bone, called corpectomy or partial corpectomy, is necessary to achieve decompression of the spinal cord.
Anterior-posterior fusion
For more severe cases, particularly multi-level compression with instability or significant kyphotic alignment, we sometimes need to decompress and stabilize from both the front and the back. This is a bigger surgery with a longer recovery, but in certain patients it’s the only way to adequately decompress the cord and maintain spinal alignment.
Posterior laminoplasty
When the compression spans multiple levels and the cervical spine has maintained its normal lordotic curve (forward curve), we can open up the spinal canal from the back by hinging open the lamina rather than removing it entirely. Laminoplasty preserves more motion than a posterior fusion and avoids the need to approach from the front. It’s a good option for patients with three or more levels of stenosis who have preserved alignment.
The choice between these approaches is driven by anatomy, not preference. I’ll walk you through the imaging and explain why one approach fits your situation better than the others.

Are you ready to meet a leading Orange County Neurosurgeon?
What to expect if you don’t have surgery
For patients with mild myelopathy who don’t yet meet surgical criteria, I recommend close monitoring. That means ongoing follow up with neurological exams, a repeat MRI if symptoms change, and a clear understanding of what red flags to watch for: worsening hand function, new balance problems, difficulty walking, or bladder changes. Activity modification is reasonable, particularly avoiding high-risk activities like contact sports or activities with a significant fall risk. But I don’t tell patients to stop living their lives. Reasonable activity and exercise are important for overall health and don’t accelerate myelopathy.
If at any point the trajectory changes, we revisit the surgical conversation.

Why Choose Dr. Alexander Taghva
Dr. Alexander Taghva is a leading board-certified neurosurgeon, specializing in brain surgery, endoscopic spine surgery, as well as spine disorders. Also, he is the only spine surgeon in Orange County and southern California who offers endoscopic laminotomy surgery. Dr. Taghva:
- Graduated from Johns Hopkins University School of Medicine and completed his residency at the University of California
- Completed a prestigious fellowship at The Ohio State University in Neuromodulation and Functional Neurosurgery
- Specializes in minimally invasive and endoscopic surgery, spinal stenosis, artificial disc replacement, spinal disorders, spinal surgery revision, and other spinal conditions.
- Specializes in brain surgery to treat trigeminal neuralgia, brain tumors, pituitary tumors, and Parkinson’s disease.
- A highly-respected neurosurgeon with many years of experience, including treating chronic pain via stimulation of the spinal cord and brain
- Actively involved in medical research and the lead investigator for clinical trials on spinal cord stimulation