




When a laminotomy works and when it doesn’t
I’m a proponent of minimally invasive surgery, but I’m more of a proponent of effective surgery. One of my mentors used to call it “minimally effective surgery” when surgeons prioritized a small incision over a complete operation. That stuck with me. If I don’t think the objectives of surgery can be safely achieved through a minimally invasive approach, I simply won’t offer it. Some patients don’t like hearing that. But I’ve found that patients like it even less when they don’t get better after surgery, or when they have a complication that could have been avoided with a more appropriate approach.
The procedure works best at segments where the lamina is wide enough to allow adequate decompression of the lateral recess without compromising the structural integrity of the spine. In practice, this usually means L4-5 and L5-S1. At these levels, the anatomy gives me enough room to work through a small window, decompress the nerve root fully, and leave the facet joint and midline structures intact.
At higher lumbar levels, the lamina tends to be narrower, and achieving a complete decompression through a minimally invasive approach can be more challenging. That doesn’t mean it’s impossible, but it changes the calculation. If I can’t adequately decompress the nerve through a small approach, a larger approach or a different procedure may be more appropriate. I’d rather do the right operation through a bigger incision than an incomplete operation through a small one.
This is the kind of detail that doesn’t show up on most “minimally invasive spine surgery” pages, but it matters. The value of MIS isn’t the small incision. It’s whether the small incision lets you do a complete job.
Synovial cysts: a special case
One condition I see frequently that’s worth addressing specifically is lumbar synovial cysts. These are fluid-filled cysts that arise from the facet joint and can compress the nerve root, causing leg pain and stenosis symptoms. They often respond well to laminotomy and cyst removal.
But here’s the nuance: a synovial cyst usually forms because the facet joint is unstable. The joint moves more than it should, the capsule gets irritated, and the cyst develops as a response. That means removing the cyst addresses the symptom, but it doesn’t fix the underlying instability. In some patients, the cyst recurs.
I don’t think every synovial cyst needs a fusion. In a patient with a stable spine, no spondylolisthesis, and a cyst causing clear radiculopathy, a laminotomy and cyst excision is a reasonable first step. It’s a same-day procedure with a fast recovery, and many patients do well long-term.
But in a patient who has a spondylolisthesis, where the vertebra is slipping forward on the one below it, the instability is the root cause. Removing the cyst without addressing the slip means the cyst is likely to come back, or the stenosis will recur from continued abnormal motion. In those patients, a fusion at the time of decompression is a better long-term decision.
This is a judgment call, and it’s one that should be made with your surgeon based on your specific imaging and symptoms. I lay out the options honestly and let the patient participate in the decision.
Call today to schedule your consultation
What the procedure involves
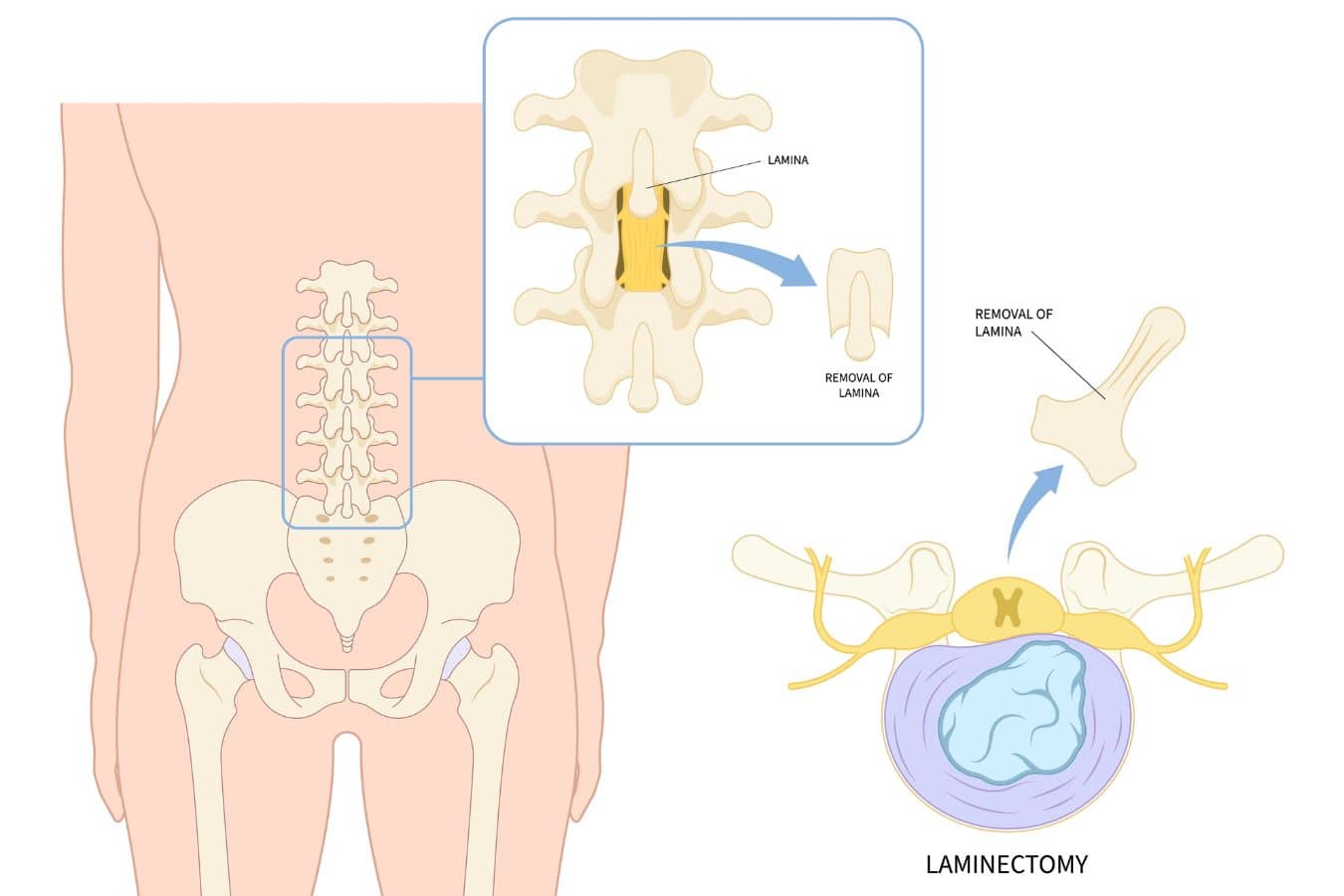
The surgery takes about an hour for a single level. Through an incision roughly the width of a finger, I place a tubular retractor to create a working channel to the spine. Using a microscope or endoscope for magnification and illumination, I remove a small window of the lamina and any thickened ligament, then decompress the nerve root by removing bone spurs, disc material, or cyst. The surrounding muscles are dilated rather than cut, which preserves the posterior musculature.
Most patients go home the same day. Pain at the incision site is typically managed with over-the-counter medication within a few days. I encourage walking immediately. Most patients return to desk work within one to two weeks and full activity by six weeks.
Testimonials
-

- James G.



Preserving the multifidus
One of the reasons I prefer minimally invasive approaches when the anatomy allows it is muscle preservation. The multifidus, the deep stabilizing muscle that runs along the spine, is stripped and retracted in traditional open surgery. That retraction can damage the muscle and its nerve supply, contributing to post-operative weakness and long-term instability.
Minimally invasive techniques use dilation rather than stripping, which is better for the muscle. But the key variable may not be the muscle itself. It may be the medial branch of the dorsal ramus, the small nerve that controls the multifidus. These nerves are difficult to see and identify during surgery, even with magnification, and they can be stretched or injured during any posterior approach. If the nerve is damaged, the muscle loses its signal regardless of how gently you treated the tissue around it.
This is also one of the reasons I have reservations about radiofrequency ablation of the medial branch nerve as a long-term pain management strategy. RFA is commonly used to treat facet joint pain by burning the same nerve that controls the multifidus. It works for pain, and symptom relief generally lasts six months to a year before the nerve regenerates and symptoms return. But during that window, the multifidus is without its control signal. We know from RFA that the nerve does come back, which is reassuring, but the question of whether repeated cycles of denervation and regeneration affect the muscle over time is still an open area of research. It’s a trade-off that I think deserves more attention than it gets.
Regardless of the surgical approach, I’m a proponent of early postoperative rehabilitation focused on multifidus reactivation. The surgery addresses the structural problem. Getting the stabilizer back online is a separate job, and it starts in the weeks after the operation.

Why Choose Dr. Alexander Taghva
Dr. Alexander Taghva is a leading board-certified neurosurgeon, specializing in brain surgery, endoscopic spine surgery, as well as spine disorders. Also, he is the only spine surgeon in Orange County and southern California who offers endoscopic laminotomy surgery. Dr. Taghva:
- Graduated from Johns Hopkins University School of Medicine and completed his residency at the University of California
- Completed a prestigious fellowship at The Ohio State University in Neuromodulation and Functional Neurosurgery
- Specializes in minimally invasive and endoscopic surgery, spinal stenosis, artificial disc replacement, spinal disorders, spinal surgery revision, and other spinal conditions.
- Specializes in brain surgery to treat trigeminal neuralgia, brain tumors, pituitary tumors, and Parkinson’s disease.
- A highly-respected neurosurgeon with many years of experience, including treating chronic pain via stimulation of the spinal cord and brain
- Actively involved in medical research and the lead investigator for clinical trials on spinal cord stimulation